Table of Contents >> Show >> Hide
- What Is Glioblastoma, And Why Is It So Difficult To Treat?
- The Breakthrough: A New Kind Of CAR-T Cell Therapy
- What Happened In The Early Trial?
- Why This Breakthrough Matters
- Mass General Is Not The Only Team Seeing Promise
- How CAR-T For Glioblastoma Is Different From CAR-T For Blood Cancer
- Is This A Cure For Glioblastoma?
- What Patients And Families Should Understand
- Why The Science Is So Encouraging
- Experience-Based Reflections: What This Breakthrough Feels Like From The Human Side
- Conclusion
Every now and then, medical science delivers a headline that sounds like it wandered in from a superhero movie, wearing a lab coat and carrying MRI scans. One of those moments arrived when early results from a new glioblastoma treatment showed a patient’s brain tumor nearly disappear within days after a single experimental cell therapy infusion.
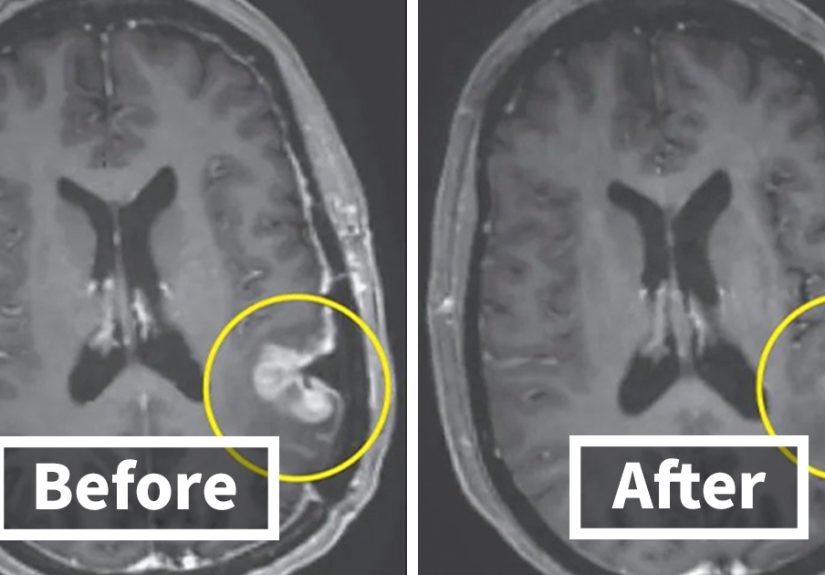
The breakthrough involved a next-generation form of CAR-T cell therapy called CARv3-TEAM-E, tested in a small, first-in-human phase 1 clinical trial at Mass General Cancer Center. The most attention-grabbing case was a 57-year-old woman with recurrent glioblastoma whose MRI, five days after treatment, showed near-complete tumor regression. Another patient had measurable shrinkage within two days, followed by a larger reduction over time. For a disease as aggressive and stubborn as glioblastoma, that kind of speed made researchers, doctors, and understandably the internet, sit up straighter.
But before anyone starts printing “cancer defeated” T-shirts, the story needs both excitement and caution. This was an early trial involving only a few patients. The responses were dramatic, but not always durable. In other words, the science is thrilling, but the finish line is still somewhere down the road, probably hiding behind a stack of peer-reviewed papers.
What Is Glioblastoma, And Why Is It So Difficult To Treat?
Glioblastoma, often shortened to GBM, is the most aggressive malignant brain tumor in adults. It grows quickly, spreads through brain tissue in a fingerlike pattern, and often returns even after surgery, radiation, and chemotherapy. Unlike a tidy tumor that sits in one neat lump, glioblastoma behaves more like glitter spilled on carpet: even when you clean up most of it, tiny bits can remain where you really do not want them.
Standard treatment usually begins with surgery when possible. The goal is to remove as much tumor as safely as the neurosurgeon can without harming important brain functions. After surgery, many patients receive radiation therapy and the chemotherapy drug temozolomide. Some may also use tumor treating fields, a device-based therapy that uses electric fields to interfere with cancer cell division. These treatments can extend survival and improve quality of life, but glioblastoma remains extremely hard to cure with today’s tools.
The challenge is not that researchers have been politely ignoring GBM. Quite the opposite. Scientists have thrown a full medical toolbox at it: targeted drugs, vaccines, gene therapies, immunotherapies, oncolytic viruses, and new delivery methods. GBM simply happens to be a ruthless opponent. It changes, hides, resists, and creates an immune-suppressing environment around itself. In the world of oncology, glioblastoma is not just a difficult boss level; it is the boss level that keeps updating its own cheat codes.
The Breakthrough: A New Kind Of CAR-T Cell Therapy
CAR-T cell therapy is a type of immunotherapy that uses a patient’s own T cells, which are immune cells that help recognize and destroy abnormal cells. In a typical CAR-T process, T cells are collected from the patient, genetically modified in a lab so they can recognize a cancer target, multiplied, and returned to the body. Once infused, the engineered cells act like highly trained security guards with a very specific wanted poster.
CAR-T therapy has already transformed treatment for some blood cancers, including certain leukemias, lymphomas, and multiple myeloma. However, success in solid tumors, such as brain tumors, has been much harder. Solid tumors are physically complex, biologically diverse, and often surrounded by defenses that prevent immune cells from working properly.
The Mass General approach, CARv3-TEAM-E, was designed to address one of the biggest problems in glioblastoma: tumor heterogeneity. That phrase sounds like it belongs in a graduate exam, but the idea is simple. Not all cells in a glioblastoma tumor are identical. If a therapy targets only one marker, some cancer cells may not carry that marker and can escape. CARv3-TEAM-E aims at more than one target by combining CAR-T engineering with a T-cell-engaging antibody molecule, or TEAM, to help recruit immune attack against a broader population of tumor cells.
What Happened In The Early Trial?
The early results came from the INCIPIENT trial, a phase 1 study evaluating CARv3-TEAM-E T cells in patients with recurrent glioblastoma. Phase 1 trials are mainly designed to study safety, dosing, and feasibility. They are not meant to prove that a treatment works for everyone. Still, when tumors shrink dramatically in days, people tend to notice.
The patient whose tumor almost disappeared
In one widely reported case, a 57-year-old woman received a single infusion of the engineered cells. Five days later, MRI imaging showed near-complete tumor regression. That does not mean every cancer cell was proven gone, and it does not mean the disease was cured. MRI scans show changes in visible tumor size and enhancement, not a magical “all clear forever” certificate. But in recurrent glioblastoma, a near-complete radiographic response within days is extraordinary.
Another patient saw rapid shrinkage
A 72-year-old man in the same early report also received a single infusion. Two days later, imaging showed an 18.5% decrease in tumor size. By day 69, the tumor had decreased by more than 60%, and the response lasted more than six months. For recurrent GBM, where tumor regrowth can happen quickly and treatment options are limited, that kind of temporary disease control can be deeply meaningful.
The important caution
Researchers also reported that tumor progression eventually occurred in the initial patients. The responses were rapid, but in several cases they did not last. One reason may be that the engineered CAR-T cells did not persist long enough in the body. Future strategies may include repeat infusions, preconditioning chemotherapy, better cell designs, or combinations with other therapies to make responses more durable.
Why This Breakthrough Matters
The reason this story created so much excitement is not simply that a tumor shrank. Tumors sometimes shrink with treatment. The surprising part was the speed, the disease type, and the fact that this happened in recurrent glioblastoma, where progress has historically been painfully slow.
For years, researchers have hoped immunotherapy could work against GBM, but the results have often been modest. Checkpoint inhibitors, which have changed outcomes in cancers such as melanoma and lung cancer, have not produced the same broad success in glioblastoma. The brain’s unique immune environment, the blood-brain barrier, tumor heterogeneity, and GBM’s immune-evasion tactics all complicate treatment.
This new wave of CAR-T research suggests that direct delivery into the central nervous system and multi-target cell engineering may help overcome some of those barriers. Instead of sending immune cells on a long commute through the bloodstream and hoping they find parking near the tumor, researchers are testing ways to place them closer to the action.
Mass General Is Not The Only Team Seeing Promise
Other researchers have been exploring similar ideas. At Penn Medicine, scientists tested a dual-target CAR-T therapy aimed at EGFR and IL13Rα2, two proteins commonly found in glioblastoma. Early phase 1 results showed reduced tumor size in all six patients shortly after treatment, with some responses lasting for months. Later data from a larger group found that tumors shrank in a portion of patients who had measurable tumor remaining after surgery.
These results do not prove that CAR-T is ready to become the new standard treatment for glioblastoma. They do show that engineered immune cells can reach brain tumors, trigger measurable activity, and in some patients create dramatic radiographic responses. That is a big deal. In cancer research, “promising” gets overused almost as much as “revolutionary,” but here the word earns its lab goggles.
How CAR-T For Glioblastoma Is Different From CAR-T For Blood Cancer
CAR-T therapy for blood cancers often targets markers found on malignant blood cells, such as CD19 or BCMA. Blood cancers are more accessible to immune cells circulating in the body. Glioblastoma, on the other hand, lives inside the brain, grows into surrounding tissue, and contains a mixed population of cancer cells. It also surrounds itself with cells and signals that can weaken immune attack.
That is why researchers are testing special delivery methods, including intraventricular or intrathecal delivery, which place treatment into fluid spaces connected to the brain and spinal cord. The goal is to bring engineered immune cells closer to the tumor and improve the odds that they can do their job.
There are also safety concerns. When immune cells become highly active in or near the brain, doctors must watch carefully for inflammation, swelling, neurotoxicity, fever, and other complications. CAR-T is not a casual “take two and call me in the morning” therapy. It requires specialized medical centers, careful monitoring, and expert teams ready to manage side effects.
Is This A Cure For Glioblastoma?
No. At least, not yet. The early results are exciting, but they do not show a proven cure. The trial involved a small number of patients, and some tumors eventually progressed. Larger trials are needed to determine who benefits, how long responses last, what dose is safest, whether repeat dosing helps, and whether treatment improves overall survival.
That said, “not a cure yet” should not be confused with “not important.” Many major cancer advances began as small, carefully watched signals in early trials. The first signs are often imperfect. Researchers then refine the treatment, study patterns, adjust dosing, combine therapies, and test the approach in more patients. Science rarely arrives like a lightning bolt. More often, it shows up with spreadsheets, cautious optimism, and someone saying, “Well, that was unexpected.”
What Patients And Families Should Understand
For patients and families facing glioblastoma, headlines about a tumor nearly disappearing can bring hope, but also emotional whiplash. Hope is powerful. Hype can be harmful. The healthiest way to read this news is: a real scientific advance has shown dramatic early activity, but it remains experimental and is not available as a routine treatment for every patient.
Anyone diagnosed with glioblastoma should speak with a neuro-oncology team about standard care, molecular testing, clinical trials, and supportive care options. Clinical trial eligibility can depend on tumor type, recurrence status, prior treatments, tumor location, genetic markers, general health, and trial-specific criteria. In other words, Google may start the conversation, but it should not be the oncologist. Google has many talents; safely treating brain cancer is not one of them.
Why The Science Is So Encouraging
The most encouraging part of this breakthrough is that it gives researchers a visible signal: engineered immune cells can produce fast tumor regression in recurrent glioblastoma. That signal creates a foundation for better questions. Can the response be extended? Can the cells be made to persist longer? Can multiple targets prevent escape? Can therapy be used earlier, when the tumor burden is lower? Can doctors predict which patients are most likely to respond?
These are not small questions, but they are the right ones. They move the field away from vague hope and toward measurable next steps. If future trials can improve durability and survival, CAR-T for glioblastoma could become one of the most important developments in brain cancer treatment.
Experience-Based Reflections: What This Breakthrough Feels Like From The Human Side
To understand why this story matters so much, it helps to think beyond the scan. Glioblastoma is not just a diagnosis written in a chart. It changes calendars, families, conversations, and the ordinary rhythm of life. A person may go from planning vacations, work projects, or dinner on Friday to suddenly learning new words like biopsy, edema, radiation mask, temozolomide, recurrence, and clinical trial. Nobody asks to become fluent in cancer vocabulary, yet many families do it overnight.
In that reality, news of a tumor almost disappearing in days lands with enormous emotional force. For a patient, it can sound like a door opening in a hallway that had very few doors. For a spouse, parent, sibling, or child, it can feel like oxygen after holding their breath for too long. Even a temporary response can matter. Extra months with stable disease can mean birthdays attended, graduations seen, hands held, jokes shared, and ordinary breakfasts that suddenly become precious.
At the same time, families who have lived with glioblastoma often develop a careful kind of hope. They know the disease can be cruelly unpredictable. They have seen treatments help and then stop helping. They may read a headline and feel both excitement and caution in the same heartbeat. That reaction is not pessimism. It is wisdom earned the hard way.
One practical lesson from this breakthrough is the importance of specialized care. Glioblastoma treatment is complex, and clinical trials often require coordination among neurosurgeons, neuro-oncologists, radiation oncologists, radiologists, pathologists, nurses, cell therapy specialists, and caregivers. The “team” in CAR-TEAM feels fitting because no patient gets through this world alone. The science may be futuristic, but the care is deeply human.
Another lesson is that patients and families should ask informed questions. Is molecular testing available? Has the tumor been checked for markers that may affect treatment options? Are there clinical trials for newly diagnosed or recurrent GBM? What symptoms should trigger an urgent call? What supportive care can help with seizures, swelling, fatigue, mood changes, speech issues, or mobility? Good questions do not guarantee perfect answers, but they help patients stay active in decisions during a time when life can feel hijacked.
There is also an emotional experience that deserves honesty: breakthroughs can be hard to read about when someone you love did not have access to them. Medical progress can feel unfair because it arrives too late for many people. That sadness is real. But each trial participant, each donated tissue sample, each family who says yes to research, helps move the field forward. The near-disappearing tumor in this story is not only a scientific image; it is a glimpse of what years of courage, funding, laboratory work, and patient participation can make possible.
So yes, this breakthrough is worth celebrating. Carefully. It is not time to declare victory over glioblastoma. It is time to recognize that a disease long known for shutting doors may have met a new kind of key. The key still needs shaping, testing, and proving. But for once, the lock moved.
Conclusion
The story of a glioblastoma patient whose tumor almost disappeared within days after experimental CAR-T therapy is one of the most striking recent developments in brain cancer research. The treatment, CARv3-TEAM-E, represents a new attempt to outsmart glioblastoma by targeting more than one tumor marker and bringing engineered immune cells closer to the brain tumor environment.
The results are early, small, and not yet durable enough to be called a cure. Still, they are scientifically meaningful. In a cancer where progress has often come slowly, rapid tumor regression after a single infusion gives researchers a powerful reason to keep pushing. For patients and families, the right takeaway is cautious hope: this is not standard treatment today, but it may help shape the next generation of glioblastoma therapy.






