Table of Contents >> Show >> Hide
- What Is Oropharyngeal Cancer (and How Is It Different From “Mouth Cancer”)?
- Causes and Risk Factors
- Symptoms: What to Watch For
- When to See a Doctor (Without Panicking)
- How Oropharyngeal Cancer Is Diagnosed
- Treatment Options
- Side Effects and Supportive Care (Because Quality of Life Matters)
- Prognosis and Survival: What the Numbers Can (and Can’t) Tell You
- Prevention and Risk Reduction
- Quick FAQ
- Real-World Experiences: What Patients and Caregivers Often Describe (Added Detail)
- Conclusion
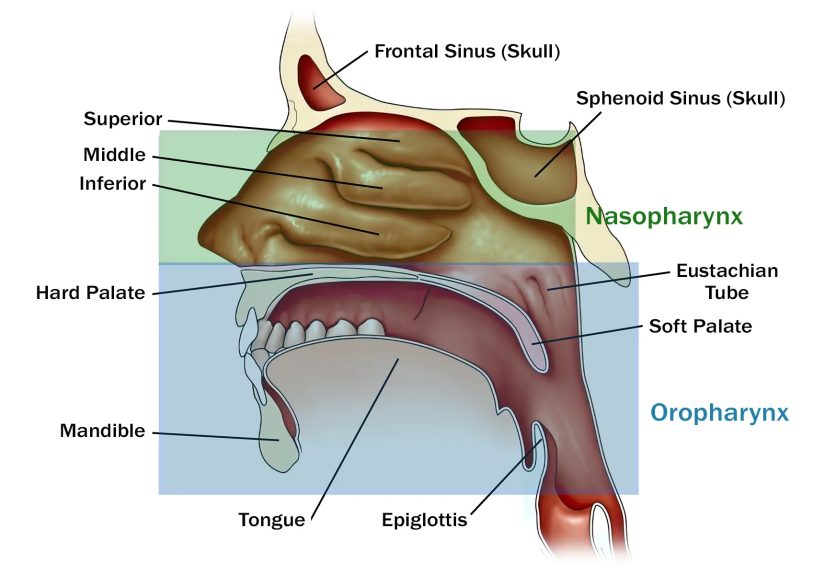
Your oropharynx (say it with me: OR-oh-FAIR-inks) is the “middle hallway” of your throatright behind your mouth.
It includes the tonsils, the base of the tongue, the soft palate, and the side/back walls of the throat. Most days, it’s busy doing boring-but-important things
like swallowing, speaking, breathing, and stopping you from inhaling a pretzel crumb the wrong way.
Oropharyngeal cancer happens when cells in that area begin growing out of control. The headline reason this cancer has changed over the last few decades?
Human papillomavirus (HPV). In the U.S., HPV is thought to cause about 60–70% of oropharyngeal cancers. Tobacco and heavy alcohol use are still major risk factors, too.
The good news: treatment has advanced a lot, and outcomesespecially for HPV-related casescan be very good when it’s found and treated appropriately.
What Is Oropharyngeal Cancer (and How Is It Different From “Mouth Cancer”)?
Oropharyngeal cancer is a type of head and neck cancer that starts in the oropharynx.
Many cases are squamous cell carcinomas, meaning they begin in the thin, flat cells lining the throat.
It’s often lumped into “oral cavity and oropharyngeal cancers,” but location matters. Cancers of the oral cavity start in places like the lips,
front of the tongue, gums, and the inside of the cheeks. Oropharyngeal cancers start farther backespecially in the tonsils and base of tongue.
That matters because causes, staging, and treatments can differ.
Causes and Risk Factors
1) HPV infection (especially HPV-16)
HPV is a common virus; many people are exposed at some point. Most infections clear on their own.
But certain “high-risk” typesespecially HPV-16can persist and, years later, contribute to cancer development in the oropharynx.
HPV-related oropharyngeal cancers often behave differently than tobacco-related cancers, and they frequently have better treatment responses.
2) Tobacco use
Smoking (and other tobacco use) increases risk. Tobacco also raises the risk of second cancers and can worsen treatment side effects.
If you needed a non-judgmental reason to quit: some evidence suggests radiation treatment works better when people stop smoking before beginning therapy.
3) Heavy alcohol use (especially combined with tobacco)
Alcohol is a risk factor on its own, but the combination of heavy alcohol use plus tobacco is particularly harmful to the tissues of the mouth and throat.
4) Other factors that can play a role
- Age and sex: These cancers are more common in men than women in the U.S.
- Immune suppression: A weakened immune system may increase risk.
- Prior head/neck cancers: A history of related cancers can raise future risk.
Symptoms: What to Watch For
Oropharyngeal cancer symptoms can be sneaky, and some people have no obvious symptoms at first.
Others notice “ordinary” throat issues that just don’t quit. A helpful rule of thumb: if something lasts more than 2–3 weeks or keeps worsening, it deserves a medical check.
Common symptoms
- Persistent sore throat
- Difficulty swallowing (or pain when swallowing)
- Earaches/ear pain (sometimes on one side)
- Hoarseness or voice changes
- A lump in the neck (swollen lymph node)
- Unexplained weight loss
- A feeling that something is “stuck” in the throat
A note that surprises many people: with HPV-related oropharyngeal cancer, a painless neck lump can be one of the first noticeable signsbecause lymph nodes
may enlarge even when the primary tumor is small and hard to see.
When to See a Doctor (Without Panicking)
Most sore throats are caused by infections, allergies, reflux, or “my heater is turning my house into a desert.”
But get checked promptly if you have any of the following:
- Symptoms lasting longer than 2–3 weeks
- Progressively worsening swallowing trouble
- A persistent neck lump
- Unexplained weight loss
- New hoarseness that doesn’t improve
Primary care clinicians, dentists, ENT (ear-nose-throat) specialists, and head-and-neck cancer teams all play roles in evaluation and diagnosis.
If cancer is suspected, referral to specialists is importantthis is not a “let’s just see how it goes for six months” situation.
How Oropharyngeal Cancer Is Diagnosed
Diagnosis is about answering three big questions:
Is it cancer? Where exactly is it? and How far has it spread?
Typical steps
- History and physical exam: A clinician looks at the throat and feels the neck for enlarged lymph nodes.
- Scope exam (often flexible nasopharyngoscopy): A thin, flexible camera helps visualize areas that are hard to see in a mirror.
- Biopsy: A tissue sample confirms cancer type. This is the “yes/no” test.
- Imaging: CT, MRI, and/or PET/CT can help map tumor size, lymph node involvement, and possible spread.
- HPV testing / p16 testing: Many oropharyngeal cancers are tested for HPV-related markers because it can affect staging and treatment planning.
Staging (the “map” that guides treatment)
Staging considers tumor size (T), lymph nodes (N), and distant spread (M). HPV-related cases may be staged differently than HPV-negative cases.
Don’t be alarmed if you hear staging terms that sound technicalyour care team should translate them into plain English and explain how they affect treatment choices.
Treatment Options
Treatment depends on the cancer’s stage, location, HPV status, overall health, and personal priorities (yes, your ability to swallow comfortably counts as a prioritybecause it is).
Many people benefit from care at centers with a dedicated multidisciplinary head and neck teamtypically including ENT/head-and-neck surgeons,
radiation oncologists, medical oncologists, radiologists, pathologists, dentists, speech-language pathologists, and dietitians.
1) Surgery
Surgery may be used for smaller, accessible tumors and sometimes for lymph nodes in the neck (neck dissection).
A major modern approach is transoral surgery, which can remove tumors through the mouth rather than through larger external incisions.
-
Transoral robotic surgery (TORS): A minimally invasive technique using robotic instruments and 3D visualization to reach “tough angles”
in the back of the throat with precision. - Transoral laser microsurgery: Another minimally invasive option used in selected cases.
Depending on pathology results (margins, lymph node involvement, and other features), surgery might be followed by radiation or chemoradiation.
2) Radiation therapy
Radiation can be used alone for some early cancers or combined with chemotherapy for more advanced disease.
Modern techniques like IMRT (intensity-modulated radiation therapy) aim to target the tumor while limiting damage to nearby healthy tissue.
Some treatment plans use different fractionation schedules (how doses are split across days), based on tumor features and clinical judgment.
3) Chemotherapy (often with radiation)
For many locally advanced oropharyngeal cancers, chemoradiation is a standard approach.
Common chemo drugs used in treatment planning can include agents like cisplatin (among others), chosen based on a person’s health, kidney function, hearing considerations, and overall risk profile.
4) Targeted therapy
Targeted therapy uses drugs designed to attack specific features of cancer cells. For oropharyngeal cancer, an example is cetuximab,
which may be used in certain recurrent or metastatic settings.
5) Immunotherapy
Immunotherapy helps the immune system recognize and attack cancer cells. In recurrent or metastatic oropharyngeal cancer, drugs such as
pembrolizumab and nivolumab are used in appropriate situations. Your clinician may also recommend biomarker testing to help predict who is most likely to benefit.
6) Clinical trials
Clinical trials may offer access to newer therapies or approachessometimes aimed at maintaining excellent cancer control while reducing long-term side effects.
Many major guidelines and cancer organizations encourage considering clinical trials when available and appropriate.
Side Effects and Supportive Care (Because Quality of Life Matters)
Treatment can be highly effective, but the oropharynx is a “high-traffic area,” so side effects deserve serious planning.
Supportive care is not an afterthoughtit’s part of the treatment.
Common side effects (vary by treatment)
- Dry mouth (xerostomia)
- Taste changes and appetite changes
- Sore throat and mouth irritation during radiation
- Swallowing difficulty (temporary or sometimes longer-term)
- Fatigue
- Skin irritation in treated areas
- Thyroid changes after neck radiation: If the thyroid area receives radiation, hypothyroidism risk increasesso thyroid blood tests before and after treatment may be recommended.
Support that can make a real difference
- Speech and swallowing therapy: Helps maintain and rebuild function during and after treatment.
- Nutrition support: A dietitian can help you keep calories and protein upcrucial for healing.
- Dental care: Dental evaluation before radiation can help prevent complications and protect teeth and jaw health.
- Smoking cessation support: Quitting improves overall health and may improve treatment response.
- Pain and symptom management: Modern supportive care can make treatment more tolerable than many people expect.
Prognosis and Survival: What the Numbers Can (and Can’t) Tell You
Prognosis depends on stage, HPV status, smoking history, overall health, and how the tumor responds to treatment.
In general, HPV-positive oropharyngeal cancers tend to have better outcomes than HPV-negative cancers, but “better” doesn’t mean “no big deal.”
It means treatment has a strong chance of success, especially when care is timely and well-coordinated.
You’ll see survival statistics reported by how far cancer has spread (localized, regional, distant). These are population-level averagesnot personal predictions.
Your doctor can explain what your stage and tumor features suggest for your individual situation.
Prevention and Risk Reduction
HPV vaccination
The HPV vaccine protects against the HPV types that cause most HPV-related cancers, including many oropharyngeal cancers.
It’s most effective when given before exposure to the virus, which is why it’s routinely recommended for preteens (with catch-up vaccination for many others).
Don’t smoke (and avoid secondhand smoke)
If you smoke, quitting is one of the most powerful risk-reduction steps you can takefull stop.
Limit alcohol
Reducing heavy alcohol use lowers risk, especially when combined with avoiding tobacco.
Regular checkups and “persistent symptoms” awareness
There isn’t a standard screening test for oropharyngeal cancer like there is for cervical cancer.
But regular dental/medical visits and paying attention to symptoms that persist can help catch problems earlier.
Quick FAQ
Is oropharyngeal cancer contagious?
Cancer isn’t contagious. HPV is a virus that can spread through intimate contact, but having HPV does not mean you will get cancer.
If my cancer is HPV-positive, does that change treatment?
HPV status can affect staging and treatment planning. Many HPV-positive cases respond well to standard therapies,
and research continues on how to keep cure rates high while reducing long-term side effects for selected patients.
Can HPV vaccination treat existing cancer?
Vaccines prevent infection; they don’t treat existing cancers. But vaccination can still be important for broader cancer prevention at the population level,
and clinicians may recommend it for eligible people depending on age and circumstances.
Real-World Experiences: What Patients and Caregivers Often Describe (Added Detail)
The medical facts matter, but so does the lived experiencethe part that doesn’t fit neatly into a staging chart.
While every person’s story is different, people facing oropharyngeal cancer often report a similar emotional arc:
confusion at the beginning, a sudden rush of appointments, then a “new normal” that evolves week by week.
Many patients describe the first symptom as something easy to dismiss. A sore throat that “should’ve been gone by now.”
A voice that sounds raspy and tired. A weird feeling when swallowing that comes and goes. For HPV-related cases, some people are surprised that the first obvious sign
is a neck lump that doesn’t hurtso it doesn’t feel urgent. A common experience is getting treated for reflux or infections first, then realizing
the symptoms are persistent enough to deserve specialist evaluation. The turning point is often an ENT visit and a scope exam where someone finally says,
“We need to look closer.”
Once a diagnosis is confirmed, many people describe the planning phase as intense but reassuring. It can feel like a small army suddenly shows up:
surgeons, radiation oncologists, medical oncologists, dentists, speech-language pathologists, dietitians. The most helpful experiences tend to happen when
the team explains not just “what we’re doing,” but “why we’re doing it this way”and how they’re going to protect swallowing, speech, and long-term quality of life.
People often say it helps to bring a notebook (or a friend who takes notes), because it’s hard to remember everything when your brain is busy quietly yelling,
“Wait, did they just say chemotherapy?”
During treatment, practical challenges often take center stage. With radiationespecially combined with chemopatients frequently talk about fatigue that feels
different from normal tiredness, plus mouth/throat soreness, taste changes, and dry mouth. Eating can become more “strategy” than “pleasure,” and many people
find themselves celebrating small wins: finishing a smoothie, keeping weight stable, getting enough protein, or making it through a week of appointments.
This is where supportive care shines. Patients often say swallowing therapy exercises feel annoying in the moment but pay off later. Nutrition support can be
a game-changer, especially when appetite disappears or food tastes “off.” Some people need temporary feeding support; those who do often describe it as a tool
that protects strength and helps them stay on track with treatmentnot as a personal failure.
After treatment, many describe recovery as a longer timeline than expected. Scans may show great results while symptoms take time to improve.
People often talk about rebuilding stamina, gradually expanding food textures, managing dry mouth, and working through anxiety before follow-up visits.
Caregivers frequently describe their own emotional whiplash: they’re relieved treatment is done, but they’re still watching for fatigue, mood changes, and the stress of “what’s next.”
Support groupsonline or localcan help, not because they hand out magic answers, but because they reduce isolation and offer practical tips from people who’ve been there.
A theme many survivors mention is that life after oropharyngeal cancer involves both gratitude and adjustment. Some people feel deeply motivated to quit smoking,
reduce alcohol, improve nutrition, and keep follow-up appointments. Others focus on voice/swallow rehab, dental care, and protecting sleep and mental health.
The “best” experience isn’t about being cheerful 24/7it’s about having a plan, getting the right support, and giving yourself permission to heal at your own pace.
If you or someone you love is going through this: you don’t have to be brave every minute. You just have to keep showing upand let the care team do their part.
Conclusion
Oropharyngeal cancer can sound intimidating (because it is), but it’s also a cancer where modern treatment and supportive care can make a huge difference.
Knowing the major risk factorsespecially HPV and tobaccorecognizing persistent symptoms, and getting evaluated early are practical steps that can change outcomes.
If you’re facing a diagnosis, ask questions, lean on your team, and remember: treating the cancer is the goal, but protecting your quality of life is part of the goal, too.






